
Feeling Pressure To Shorten Early Development Timelines?

Lengthy early-development timelines are common across new and emerging biotech companies for a multitude of reasons. Striking the right balance of speed, quality, risk, and investment allows you to shorten timelines and work with efficiency. Strategies adopted for a rapid development of a simple yet flexible format proves beneficial.

The cost and benefit of failure
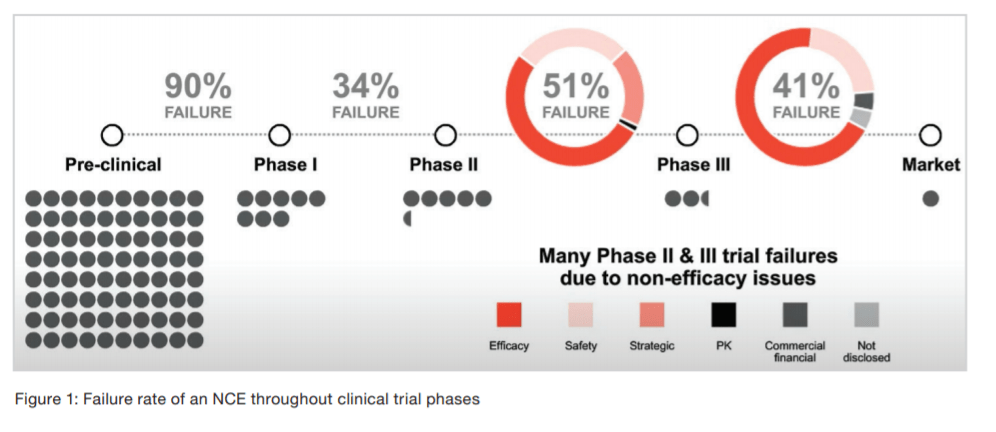
The failure rate for traditional new chemical entity (NCE) development is significantly high in the early stages of development, with 90% of NCEs failing before they even reach Phase I testing (see Figure 1) based on poor exposure or animal toxicity. Once the molecule moves from Phase I to Phase II and safety issues are addressed, the failure rate drops to 34%, and the efficacy testing of the drug candidate for the specific therapeutic indication becomes the primary goal (1). We see about half of molecules survive past Phase II, where a critical decision on go/no is done by the clinicians and sponsor companies based on investment in expensive Phase III clinical study and CMC work. From there, the rate drops again to 41%, which could be related to a variety of reasons, such as safety and/or adverse side effects that were not prominent until the drug was given to a larger patient pool. A company’s market strategy, competitive landscape in a specific therapeutic area, and business decision could also cause a program to be suspended prior to filing.
Failure during drug development, while costly and frustrating, does create opportunities to take advantage of a drug repurposing strategy (also known as drug repositioning or drug reprofiling), which redirects approved, failed, or shelved drugs and/or recycles existing compounds for novel indications. In fact, many successful drug candidates have been largely serendipitous discoveries. For example, sildenafil, which has been sold as Viagra since 2005, was tested as a treatment for erectile dysfunction only after the side effect emerged in Phase I trials for cardiovascular disease (2). The antihypertensive medication, minoxidil, was reformulated into the topical cream Rogaine after patients using it to lower blood pressure also experienced hair regrowth (3) Driven by these and other repurposing success stories, researchers are now taking more tactical approaches to pinpoint new uses for existing shelved or failed drugs and are relying on new high-throughput techniques, such as large-scale screens and bioinformatic strategies, to mine data for drug–disease connections.
The timeline and cost of developing a novel NCE only compounds the high failure rate. Between 10 and 12 years and approximately $2 billion to $3 billion is needed to discover a candidate compound and then take it through the necessary preclinical and clinical tests needed for FDA approval (4) To save money, companies, academic institutions, and even nonprofit organizations are getting into drug repurposing where a pharmaceutical company has already invested the resources for preclinical development as well as Phase I and, sometimes, Phase II and Phase III human trials. Repurposing drugs is a more time- and cost-efficient strategy as bringing a repurposed drug to market is estimated at $300 million.
Even with clinical data in hand, it is no small feat to conduct successful late-phase trials required by the FDA for approval of a new indication. In fact, these trials are arguably the most expensive phases of clinical testing, with a Phase III trial program costing anywhere between $40 million to $300 million (5). The attrition rate for repurposed drugs is estimated to be about 65% versus 90% to 95% of new chemical entities (6).
The drug repurposing development pathway
A comparison of the pathways for the traditional development of a novel drug versus that of a repurposed drug highlights the advantages of the latter (see Figure 2). For example, it is not necessary to carry out any safety studies on a repurposed drug, thereby allowing you to potentially move directly to Phase II and Phase III clinical trials (based on the specific indication). There are cases when safety studies may be required, such as when the doses are significantly higher or if the single ascending dose and multiple ascending dose studies have not yet been conducted. Nevertheless, because safety studies do not need to be conducted on repurposed drugs, the regulatory pathway can be reduced from 10 to 15 years (traditional timeline for an NCE) to about three to eight years (6) A repurposed drug is often filed under the 505(b)(2) pathway and then filed as an NDA or BLA, depending on whether it is a large or small molecule. It is currently estimated that 30% of FDA-approved, new drug products and repurposed drugs account for approximately 25% of the pharmaceutical industry’s revenue. Data published by BCC Research (see Figure 3) shows an increasing global market trend for repurposed drugs over the last several years (7).
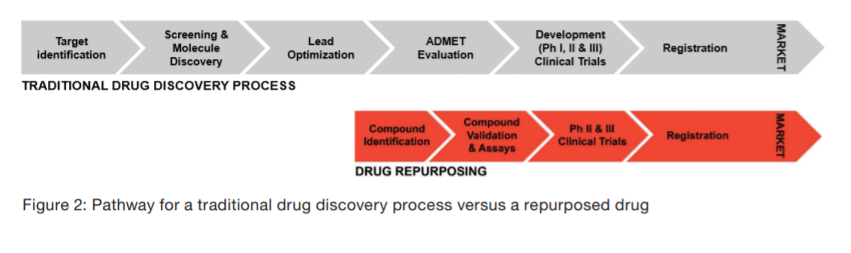
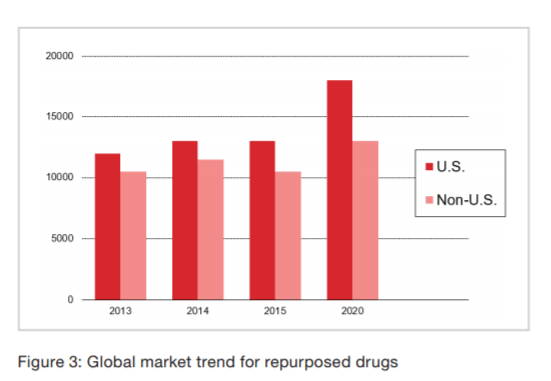
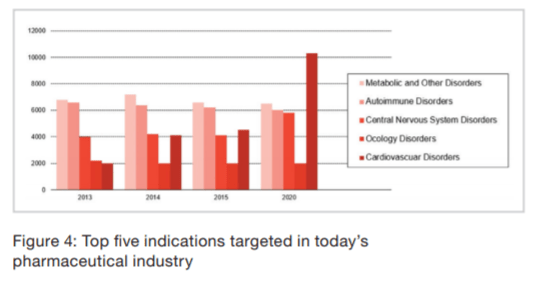
Figure 4 below shows the trends related to the application or the therapeutic category, where the top five indications stay the same, regardless of whether the drug is repurposed or an NCE (7).
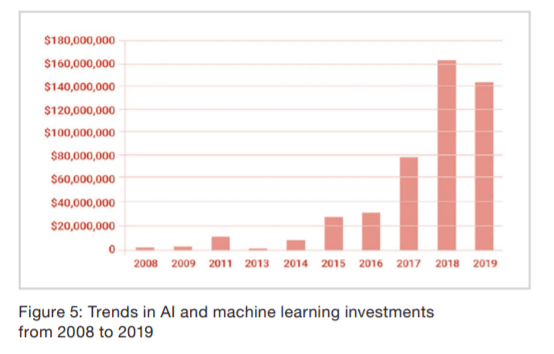
Some approaches adopted by industry experts (more so in the last five to eight years than the past 10 to 15) to identify drugs for newer indications in drug design include the use of Big Data, quantitative structured activity relationship modeling, computational tools, machine learning, neural networks, artificial intelligence, and high-power computing techniques. Researchers, medicinal chemists, and pharmaceutical experts have also adopted many other computational and experimental approaches to use in drug repurposing. Some examples include molecular docking, genetic association, phenotype screening, signature matching, and retrospective clinical analysis. There are also many companies investing in artificial intelligence as well as partnerships forming among Big Pharma and even medium-sized companies with experts who can use artificial intelligence in drug discovery. Figure 5 shows the increase in investments in artificial intelligence and machine learning over the last 10 years (8).
AstraZeneca’s new R&D framework, termed the “5Rs,” has introduced increased scientific rigor and emphasis on quality, driving an almost five-fold improvement in R&D productivity. This approach ensures each project team focuses on improving its understanding of a key set of criteria, which include the right target, tissue, safety, and patient as well as having the right commercial strategy and a unique value proposition. The results of this effort led to an improvement in its Phase II failure rate, going from 85% between 2005 and 2010 to 60% between 2012 and 2016. There was also an overall improvement in its success rate of drug candidate nomination to Phase III study completion, which went from 4% to 19% over the same timeframe (9).
There are many potential drug repurposing pathways being considered. Authorized drugs can follow different repurposing pathways, depending on whether they are still under the protection of their original patent or whether they were adapted for the new use. If commercial strategies are applicable, it is likely that the repurposed drug will be developed and registered by the pharmaceutical industry. However, other options, such as off-label use and public promotion, should be explored. Promoting or publishing the positive outcomes, experience, and data of experience of use of the drugs and smaller clinical studies will help medical professionals and the healthcare industry evaluate the use of current drugs for newer indications. If the repurposing strategy does not meet the commercial/ financial returns of investment for the pharma industry, then it is likely that the medical profession will use these studies and data for the sole benefit of the patient.
Shelved and off-label drugs
Many pharma companies shelve development programs of experimental drugs in Phase I or Phase II, and even sometimes Phase III, either because they do not work or are unsafe. In other cases, they just no longer fit a company’s strategic goals. Many companies must then prioritize these molecules to determine where investments into large-phase clinical trials should be made. This creates opportunities to out-license these molecules to smaller players, such as startup companies, as well as open the door to spinout companies or new startup entities that then look at drug repurposing independently. For example, SpringWorks is a spinout of Pfizer focused on bringing new life to shelved drugs. Another example is iOnctura, a spinout company exploring new applications for shelved immuno-oncology drug candidates.
Off-labelling drugs is another form of drug repurposing. According to the FDA, the term “off-label” can mean a drug is: (a) used for a disease or medical condition that it is not approved to treat; (b) given in a different way, e.g., a drug approved as a capsule is given as an oral solution instead; and (c) given in a different dose, e.g., a drug is approved at a dose of one tablet a day but a doctor prescribes a dose of two tablets a day (10). For example, hydroxychloroquine is an FDA-approved drug for malaria and lupus but is now an off-label drug for COVID-19. Reports show that 30% of cancer drugs and 70% of pediatric antipsychotic drugs are prescribed for off-label uses (11).
There are pros and cons, of course, to this strategy. The biggest difference is that off-label drugs are not systematically evaluated for a specific indication, thereby allowing drug repurposing companies to conduct clinical trials and include them on the new label indications for approval by a regulatory agency.
The promise of repurposed drugs
A drug repurposing strategy can result in new sales and market opportunities for shelved or abandoned compounds or drugs and, during that exploration, may also reveal major new mechanisms of action relative to new target disease indications. These discoveries could potentially lead to an intellectual property claim as well as extend the life of current marketed drugs by determining new indications and/or formulations. This depends, though, on several factors, including the component parts of the drug repurposing discovery process, the IP and the regulatory issues pertaining to the clinical trials, and suitable business models. Repurposed drug market exclusivity is of paramount importance and can also be achieved by a combination of IP and regulatory efforts executed via an appropriate business model.
In the case of NCEs, patent filing often occurs early in the discovery cycle of the candidate drug. This can result in a rather limited lifespan of composition of matter patent production for the NCE marketed drug. This is not the case with repurposed drugs. The repurposing process enables a later stage filing of a patent and significantly increases the patent protection period of repurposed drugs. Yet, the success of such a strategy will also depend on the availability of genetic products that can be substituted by off-label prescription use by individual physicians.
Market exclusivity for an orphan disease drug is particularly attractive, regardless of whether the application was filed as a 505(b)(1) or a 505(b)(2) (References 12, 13). It consists of a seven-year period that begins once the drug has been granted approval by the FDA and is independent of the drug’s current patent status. A similar provision exists for pediatric drugs, which allows for an additional six-month exclusivity period. Drug repurposing companies are predominantly focused on producing robust clinical pipelines and market-driven therapeutic drugs. The drug repurposing sector is growing rapidly with an average of 14 to 16 new companies being formed every five years (14). Exit strategies for repurposing companies by acquisition have also been enormously successful. Repurposed drugs have proven valuable in the current COVID-19 pandemic as scientists explore more than 140 drugs to combat this deadly virus. For example, drugs intended for other purposes, such as chloroquine, hydroxychloroquine, and remdesivir, are now showing promise against COVID-19. Thermo Fisher Pharma Services is proud to state that we are actively working on more than 40 programs to support our partners in the pharmaceutical industry to treat COVID-19.
Drugs repurposed over the last 5 to 10 years have covered a wide range of diseases and therapeutic categories, and there is still opportunity with many others as well. In a recent study by a joint project between Harvard, MIT, and the Dana-Farber Cancer Institute, over 4,000 drugs used to treat conditions, such as diabetes, inflammation, alcohol abuse, and arthritis in dogs, showed an “unexpectedly high rate of anti-cancer activity” (15). According to an article about the study, these medications were tested “against 578 laboratory cancer cell lines spanning 24 tumor types, resulting in the identification of 49 non-cancer drugs that selectively killed cancer cells and whose activity against cancer could be predicted using molecular biomarkers. Another 103 compounds reporting less selectivity against cancer cell lines were also identified.”
The market potential for a repurposed drug is determined by the same market forces as a conventional NCE drug and includes drug differentiation, market need, patient acceptance, marketing strategy, and IP positioning. These products have the same opportunity to achieve blockbuster status as a de novo-derived drug.
Summary
Drug repurposing constitutes anywhere from 10% to 50% of current R&D spending and is a determining factor in the life-cycle management of pharmaceutical products (6). Many large pharmaceutical companies have embraced drug repurposing in either a formal or ad hoc manner. Some companies perceive candidate compounds for a polypharmacological perspective in parallel and, therefore, for a potential treatment for multiple diseases while simultaneously running clinical studies. Others have dedicated internal resources specifically to drug repurposing or, for smaller companies, found new opportunities with shelved molecules.
Drug repurposing has gained considerable momentum in the last decade, as it offers a great business opportunity for the entire pharmaceutical industry. Not surprisingly, the strategy has just been integrated in life-cycle management of pharmaceutical products, with CDMOs playing a critical role as partners in the process by helping to quickly bring repurposed drugs to the market for the benefit of the patients and healthcare.
Learn more about our drug repurposing services.
References
- Takebe T., Imai R., Ono S. (2018). “The Current Status of Drug Discovery and Development as Originated in United States Academia: The Influence of Industrial and Academic Collaboration on Drug Discovery and Development,” Clin. Transl. Sci. 11:597–606. doi
- Dhir, Neha et. al. (April 23, 2020). “Drug Repurposing and Orphan Disease Therapeutics,” in Drug Repurposing – Hypothesis, Molecular Aspects and Therapeutic Applications.Farid A. Badria. Ed. IntechOpen. DOI: 10.5772/ intechopen.91941.
- Bryan, J. (2011). “How minoxidil was transformed from an antihypertensive to hair-loss drug.” The Pharmaceutical Journal. 287. 137-138.
- Nosengo, N. (2016). “Can you teach old drugs new tricks?” Nature. 534, 314–316.
- Azvolinksy, Anna. (January 1, 2017). “Repurposing Existing Drugs For New Indications.” The Scientist.
- Naylor, Stephen et. al. (2015). “Therapeutic Drug Repurposing, Repositioning and Rescue Part III: Market exclusivity using Intellectual Property and regulatory pathways.” Drug Discovery World.
- Walker, Nigel. (December 7, 2017). “Accelerating Drug Development through Repurposing, Repositioning, and Rescue.” Pharmaceutical Outsourcing.
- Jefferies Financial Group. (March 2, 2020). “AI and Machine Learning in Drug Development: The Decade Ahead.”
- Pangalos, Menelas al. (2018). “AstraZeneca R&D – Improving Drug Development Productivity With Better Predictivity.” Drug Discovery World.
- FDA. (February 5, 2018). Understanding Unapproved Use of Approved Drugs “Off Label.”
- McKeehan, Nick. (October 19, 2017). “Promise In Off-Label Drugs For Alzheimer’s.” Cognitive Vitality.
- EvaluatePharma®. Orphan Drug Report 2019. (November 2020). ©Evaluate Ltd. and Informa PharmaProject database.
- Drew, Angela and King, Jennifer. (April 8, 2018). “505(b)(1) versus 505(b)(2): They Are Not the Same.” Camargo Pharmaceutical Services.
- Culbertson, Adam et. al. (August 3, 2007). “Personalised Medicine – Technological innovation and patient empowerment or exuberant hyperbole?.” Drug Discovery World.
- Clinicalomics. (2020). “Drugs Developed for Other Illnesses Might Be Repurposed for Cancer Treatment.”
